Clinical evidence proves the importance of the ‘GOLDEN HOUR’ in Emergency Stroke care, but ‘Golden Hour’ is not recognised by Department of Health (DoH).
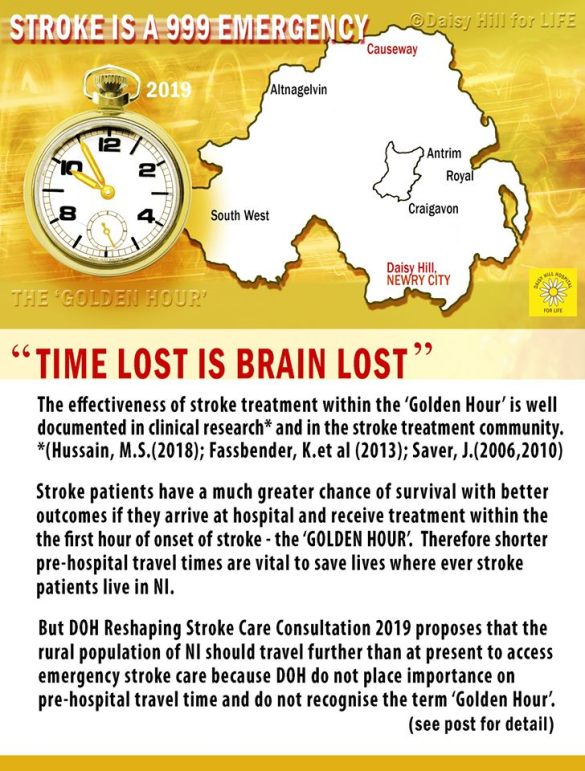
It is well known that STROKE is a 999 EMERGENCY where every second counts for the patient receiving acute stroke care and the critically time dependant clot-busting drug Alteplase used in Thrombolysis.
The options given in the 2019 Stroke consultation show clearly that the Department of Health NI are IGNORING the fact that every stroke patient, no matter where they live, needs to be seen and treated as an Acute Stroke Care 999 Emergency ideally within the ‘Golden Hour’. This means making pre hospital travel times as SHORT AS POSSIBLE, so that the patient can ideally be treated within the ‘Golden Hour ‘from onset of stroke to needle time.
Rather than make pre-hospital travel times SHORTER, the DoH are proposing to make pre hospital travel times LONGER for patients living in Newry Mourne & Down and other areas in NI.
Stroke patients who presently are scanned in Daisy Hill (and if eligible) given Thrombolysis are already immediately transferred to the Royal for Thrombectomy if suitable.
If 2019 Reshaping Stroke Care proposals go ahead, dying stroke patients WILL BE DENIED IMMEDIATE TREATMENT and have to be transferred to Craigavon, 45 minutes away (to see if they are even suitable for Thrombolysis, never mind Thrombectomy) and will have much worse outcomes due to the delay in transfer and will be denied the best chance for survival.
TIME DELAY IN GETTING 999 EMERGENCY CARE IS NOT ACCEPTABLE
It is not acceptable that people from the Rural Areas of NI who will already have travelled long distances to access existing specialist Stroke Units, (using up precious minutes of the ‘Golden Hour’ already) will have to travel even FURTHER, losing vital brain cells and causing untold brain damage on the journey. It also means that patients who suffer a stroke when in hospital or ED will be denied access to the existing specialist Acute Stroke/Rehab Unit in Newry and denied immediate treatment.
WHY IS THE FIRST HOUR TERMED ‘GOLDEN’?
The effectiveness of treatment in the GOLDEN HOUR is well documented in the emergency medicine and stroke treatment community, even if our DoH refuse to recognise the term ‘Golden Hour’ in the recent FAQ/ Frequently asked Questions supplement to the consultation document (see FAQ5).
It is well known that patients receiving treatment within the first 60
minutes of symptom onset, (termed the Golden Hour,) have the greatest
opportunity to benefit from restoration of blood flow therapy with
respect to disability and living independently. This time-frame is when
the volume of salvageable brain and the patient’s capacity to benefit
from clot-busting therapy are greatest.
The reason the first hour of stroke is called ‘golden’ is because
stroke patients have a much greater chance of SURVIVING and avoiding
long-term brain damage if they arrive at the hospital and receive
treatment with a clot-busting drug called TPA (Altepalse) within that
first hour from onset of stroke:
“Therapeutic benefit is maximal in the first minutes after symptom onset and declines rapidly during the next 4.5 hours.” (Saver MD)
DoH DO NOT RECOGNISE THE TERM ‘GOLDEN HOUR.’
The DoH try to justify selectively making Stroke patients travel further for immediate Emergency Stroke Care during the ‘Golden Hour’ from onset of stroke in Newry Mourne & Down by stating that: “the Golden Hour is not a recognised term in Stroke Care. In our healthcare system we work to the National Clinical Guidelines for stroke, which is the definitive source of how stroke care should be delivered in the UK.”
It is the DoH’s opinion that: “The most important factor in stroke care is not the time to hospital. It is the time to expert assessment, brain scanning and treatment that is critical.” (See FAQ 5:Taken from Questions and Answers Supplement to 2019 Stroke Consultation).
CLINICAL EVIDENCE SUPPORTING IMPORTANCE OF ‘GOLDEN HOUR’
At the International Stroke Conference 2018 in Los Angeles M. Shazam Hussain, MD, Director of Cleveland Clinic Cerebrovascular Center presented significant findings that the “golden hour” is proving to live up to its name, even for patients with one of the most serious forms of ischemic stroke.
According to this study, 52 percent of individuals suffering an ischemic stroke had better long-term outcomes if they received Thrombolysis medication (Alteplase) within 60 minutes of symptom onset. This compares to only 27 percent of patients showing good long-term outcomes – with respect to disability and living independently — if administered Alteplase beyond the golden hour.
A summary of The Lancet article (2013): ‘Streamlining of pre-hospital stroke management: the golden hour’ reinforces the importance of the narrow time-frame or ‘Golden Hour’:
“Thrombolysis with Alteplase administered within a narrow therapeutic window provides an effective therapy for acute ischaemic stroke. However, mainly because of prehospital delay, patients often arrive too late for treatment, and no more than 1–8% of patients with stroke obtain this treatment.
We recommend that ALL LINKS in the PREHOSPITAL STROKE RESCUE CHAIN must be optimised so that in the future more than a small minority of patients can profit from time-sensitive acute stroke therapy.”
The Lancet article (2013)
Therefore pre-hospital travel time for the Newry Mourne and Down population should also be shortened, not lengthened, in receiving 999 Emergency Stroke Care to save lives with better outcomes.

DAISY HILL, NEWRY IS THE RIGHT PLACE FOR A HYPERACUTE STROKE UNIT – A VITAL OMISSION FROM THE 6 PROPOSED 2019 STROKE CONSULTATION OPTIONS
Newry Mourne and Down – with a population of 180,000 is the third largest Local Government District population in NI. Daisy Hill Acute Hospital, Newry City with its STRATEGIC LOCATION – is the right place, entitled to have a hyperacute stroke unit co-located with an acute stroke unit.
This option will give a fair and equitable chance of survival with better outcomes for dying stroke patients in this LGD, like the population attending the Royal, Altnagelvin and Craigavon.
‘TIME LOST IS BRAIN LOST.’
The Emergency Stroke Care “Golden Hour” is already a very narrow time-frame. Additional delay in pre-hospital travel times which the DoH are selectively imposing on the Rural Catchment population of Newry Mourne and Down will cost lives, not save saves and cannot be condoned.
The population is entitled to fair and equitable treatment, so this proposal to withdraw emergency and specialist acute stroke care from the combined Specialist Acute Stroke/Rehab Unit, which has existed since pre-2003 in Daisy Hill Acute Hospital, Newry, must be challenged!
You can follow the Daisy Hill Acute Hospital campaign also by visiting and liking our Facebook page at https://www.facebook.com/daisyhillforlife/ – Thank you.
© Daisy Hill for Life on Facebook and http://www.savedaisyhillhospital.com, 2015 – 2021. We welcome sharing of this info and the use of excerpts and links, provided that full and clear credit is given to http://www.savedaisyhillhospital.com and Daisy Hill for Life with appropriate and specific direction to the original content. Thank-you!